 Calcium – A Clinically Effective Natural Remedy for PMS & PMDD?
Calcium – A Clinically Effective Natural Remedy for PMS & PMDD?
Premenstrual Syndrome (PMS) is one of the most common debilitating disorders that affects women. 95% of women of reproductive age experience premenstrual symptoms, and severe PMS symptoms, including premenstrual dysphoric disorder (PMDD), occur in 5% of these women.1
Approximately 20% of all women experience premenstrual symptoms severe enough to impair their activities of daily life.2 Thus, PMS is associated with significant discomfort and is an economic burden for individuals and populations due to absenteeism at work and other factors.3
 Menstrual Cycle Chart & PMS Symptom Review
Menstrual Cycle Chart & PMS Symptom Review
There are two phases in an ovulatory menstrual cycle – the follicular phase and the luteal phase. The luteal phase begins after ovulation, as shown in this chart:
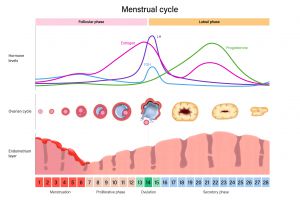 PMS symptoms begin before the menstrual period during the luteal phase of the menstrual cycle and typically resolve with menstruation, which initiates the follicular phase of the next menstrual cycle, as seen above.1
PMS symptoms begin before the menstrual period during the luteal phase of the menstrual cycle and typically resolve with menstruation, which initiates the follicular phase of the next menstrual cycle, as seen above.1
Signs and symptoms of Premenstrual Syndrome (PMS) include:
- Mood Swings
- Anxiety
- Acne or Other Skin Concerns
- Breast Pain (also known as Premenstrual Mastalgia)
- Increased Appetite
- Food Cravings
- Fatigue
- Irritability
- Anger outbursts
- Depression
- Crying or Tearfulness
- Restlessness
- Difficulty Concentrating
- Social Isolation
- Sadness
- Loneliness
- Dizziness
- Insomnia or Hypersomnia
- Changes in Libido
- More Accident-prone
- Headaches
- Migraines
- Back pain
- Muscle and Joint pain
- Abdominal Pain or Cramping
- Weight Gain
- Abdominal Bloating or Swelling
- Water Retention
- Edema of Extremities
- Sweating
- Constipation or Diarrhea
- Low Tolerance for Light and Sound
- Loss of Confidence
- Nausea1,4
 Does Calcium Relieve Premenstrual Syndrome (PMS) Symptoms?
Does Calcium Relieve Premenstrual Syndrome (PMS) Symptoms?
Fortunately, yes, there are natural remedies available that may support a healthy, asymptomatic menstrual cycle. One option to discuss with your patients is calcium. A recent systematic review compiled data from 14 clinical studies and determined serum calcium levels trend lower in women who experience PMS. The evidence analyzed also suggests calcium supplementation could significantly improve PMS symptoms via several physiologic mechanisms.3
 Sex Hormone Levels & the Regulation of Calcium Levels
Sex Hormone Levels & the Regulation of Calcium Levels
Research suggests calcium supplementation may support a healthy menstrual cycle because the sex hormones produced by the ovaries during the menstrual cycle can directly impact calcium status and the production of parathyroid hormone, which is a hormone that regulates blood calcium levels. Estrogen directly affects the movement of calcium into tissues, including muscles and bones.3
Overall, estrogen tends to lower the calcium level in the blood due to the significant effect it has on bone formation. Estrogen stimulates the mineralization of bone, which is a process that moves calcium out of the blood and into the bone.3 Progesterone also plays a role in bone formation; therefore, the natural changes in the progesterone level during a healthy ovulatory menstrual cycle may also contribute to transient shifts in calcium status.5
 Estrogen Levels During the Menstrual Cycle, Calcium Status and PMS Symptoms
Estrogen Levels During the Menstrual Cycle, Calcium Status and PMS Symptoms
In women with an underlying calcium disturbance or insufficient calcium intake, the increased sex hormone production that naturally occurs during the menstrual cycle could decrease blood calcium levels, leading to PMS symptoms.3 The reduced blood calcium level could contribute to abnormalities in brain cell activity due to changes in neurotransmitter synthesis and release.3,6
Evidence suggests that fluctuating estrogen levels may alter serotonin receptor binding and serotonin receptor availability, thereby initiating mood symptoms associated with PMS.3 Furthermore, estrogen decreases calcium entry into vascular smooth muscle cells, which could also contribute to some symptoms of PMS.3 Calcium is a mineral that plays a central role in muscle contractions; therefore, changes in calcium transport and the calcium concentration in the blood could significantly affect the neuromuscular signaling pathways.3,7
Two estrogen peaks during the menstrual cycle can significantly impact calcium levels. The estrogen peaks are illustrated by the green line in the graph below:
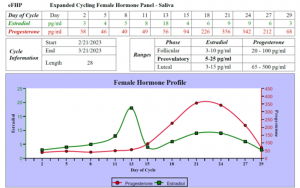
The first estrogen peak (on Day 13 above) during the menstrual cycle occurs just before ovulation, and the second estrogen peak occurs during the luteal phase after ovulation when estrogen “follows” the progesterone released from the corpus luteum in the ovary.
The natural estrogen peaks during the menstrual cycle may contribute to lower calcium concentrations in the blood, PMS symptoms, and increased parathyroid hormone levels.3,8,9
 What is Parathyroid Hormone?
What is Parathyroid Hormone?
Parathyroid hormone (PTH) is produced by the parathyroid glands, which are located behind the thyroid. PTH regulates calcium balance in the body by increasing the calcium level in the blood. PTH affects the kidneys, digestion, and bone, which play roles in maintaining an optimal blood calcium level. Specifically, PTH enhances calcium reabsorption in the kidneys to decrease the amount of calcium excreted in the urine, increases the synthesis of active vitamin D to increase the absorption of dietary and supplemental calcium in the gastrointestinal tract, and increases the breakdown of bone to increase the level of available calcium in the blood.10
 How Does Calcium Alleviate Premenstrual Syndrome (PMS) Symptoms?
How Does Calcium Alleviate Premenstrual Syndrome (PMS) Symptoms?
Calcium supplementation during the menstrual cycle may resolve an underlying calcium deficiency or insufficiency, suppress parathyroid hormone secretion, reduce neuromuscular irritability, optimize neurotransmitter signaling, and decrease vascular reactivity to improve the symptoms of PMS.3,8
Research shows a clear association between a low blood calcium level and PMS symptoms. Clinical studies confirm calcium levels are lower during the luteal phase, when PMS symptoms occur, compared to the follicular phase. Moreover, several studies demonstrate that calcium supplementation alleviates many symptoms of PMS, including mood concerns.3,8 An interesting relationship between PMS and bone loss has also been identified via research, which provides additional evidence that suboptimal calcium levels or abnormal calcium metabolism could be underlying causes of PMS.8
 How Much Calcium Does Your Patient Need Daily?
How Much Calcium Does Your Patient Need Daily?
According to the Institute of Medicine, menstruating females between the ages of 19 – 50 require 1000 mg of calcium daily from food and supplements.11 Since there is a relationship between calcium status and several other nutrients, such as magnesium and vitamin D, additional nutrients might need to be prescribed with calcium supplements to optimize calcium status.12
 What Calcium Supplement Dose is Best for Premenstrual Syndrome (PMS) Symptoms?
What Calcium Supplement Dose is Best for Premenstrual Syndrome (PMS) Symptoms?
Doctors and research scientists hypothesize that supplementation with calcium may prevent the transiently reduced calcium levels caused by the higher estrogen levels present just before and during the luteal phase of the menstrual cycle.3
Doses of calcium that are beneficial in research studies range from 500 mg – 1000 mg.13 But, based on the available evidence, it is not yet possible to suggest an optimal calcium dosage for PMS. Well-designed dose-response clinical trials with large sample sizes are needed to establish the dose of calcium most effective for supporting women with PMS symptoms.3 Consider discussing daily dietary calcium intake with your patients to determine if calcium supplementation might be supportive for those with PMS or PMDD.
 Assess the free, bioactive salivary hormone levels throughout an entire menstrual cycle with the Cycling Female Hormone Panel or the Expanded Cycling Female Hormone Panel.
Assess the free, bioactive salivary hormone levels throughout an entire menstrual cycle with the Cycling Female Hormone Panel or the Expanded Cycling Female Hormone Panel.
To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients. You may select this option at the top of the order form.
Please visit our Provider Tools page for more information about choosing the right test, test result interpretation, and treatment options.
 References:
References:
- Kwan I, Onwude JL. Premenstrual syndrome. BMJ Clin Evid. 2015;2015:0806.
- Alshdaifat E, Absy N, Sindiani A, et al. Premenstrual Syndrome and Its Association with Perceived Stress: The Experience of Medical Students in Jordan. Int J Womens Health. 2022;14:777-785. doi:10.2147/IJWH.S361964
- Arab A, Rafie N, Askari G, Taghiabadi M. Beneficial Role of Calcium in Premenstrual Syndrome: A Systematic Review of Current Literature. Int J Prev Med. 2020;11:156. doi:10.4103/ijpvm.IJPVM_243_19
- Siminiuc R, Ţurcanu D. Impact of nutritional diet therapy on premenstrual syndrome. Front Nutr. 2023;10:1079417. doi:10.3389/fnut.2023.1079417
- Seifert-Klauss V, Prior JC. Progesterone and bone: actions promoting bone health in women. J Osteoporos. 2010;2010:845180. doi:10.4061/2010/845180
- Tiranini L, Nappi RE. Recent advances in understanding/management of premenstrual dysphoric disorder/premenstrual syndrome. Fac Rev. 2022;11:11. doi:10.12703/r/11-11
- Valentim MA, Brahmbhatt AN, Tupling AR. Skeletal and cardiac muscle calcium transport regulation in health and disease. Biosci Rep. 2022;42(12):BSR20211997. doi:10.1042/BSR20211997
- Thys-Jacobs S. Micronutrients and the premenstrual syndrome: the case for calcium. J Am Coll Nutr. 2000;19(2):220-227. doi:10.1080/07315724.2000.10718920
- Thys-Jacobs S, Alvir MJ. Calcium-regulating hormones across the menstrual cycle: evidence of a secondary hyperparathyroidism in women with PMS. J Clin Endocrinol Metab. 1995;80(7):2227-2232. doi:10.1210/jcem.80.7.7608284
- Leung EKY. Parathyroid hormone. Adv Clin Chem. 2021;101:41-93. doi:10.1016/bs.acc.2020.06.005
- Office of Dietary Supplements – Calcium. NIH Office of Dietary Supplements. July 24, 2024. Accessed January 24, 2025. https://ods.od.nih.gov/factsheets/calcium-HealthProfessional/#en1.
- Khazai N, Judd SE, Tangpricha V. Calcium and vitamin D: skeletal and extraskeletal health. Curr Rheumatol Rep. 2008;10(2):110-117. doi:10.1007/s11926-008-0020-y
- Abdi F, Ozgoli G, Rahnemaie FS. A systematic review of the role of vitamin D and calcium in premenstrual syndrome [published correction appears in Obstet Gynecol Sci. 2020 Mar;63(2):213]. Obstet Gynecol Sci. 2019;62(2):73-86. doi:10.5468/ogs.2019.62.2.73