
Testosterone (T) is considered the “elixir of life” and has been sought after for its rejuvenating properties for millennia.1,2 Testicular extracts from animals were used by the ancient Chinese and the Romans for men’s health. The idea and practice of optimizing hormone levels for health benefits became more widespread when the acclaimed scientist and endocrinologist Dr. Charles Brown-Séquard regularly injected himself with testicular extracts in the late 1800s to restore vitality.1
What is Testosterone?
Testosterone (T) is derived from cholesterol (like all other steroid hormones) and is a sex hormone. Sex hormones include androgens, estrogens, and progestogens.3 T is one of the androgen hormones, and many have referred to T as the “fountain of youth.”2,4
While testosterone (T) is known as a male or masculine hormone, both women and men naturally produce T, and women are more sensitive to T. Men have approximately ten times as much T as women, and optimal T production is crucial for the health of men and women. The reproductive and adrenal glands produce most of the T in both sexes, but small amounts are also produced in the brain. Therefore, testosterone is also known as a neurosteroid.5
We primarily think of T as a reproductive hormone, but T affects all tissues that have T receptors (androgen receptors). Androgen receptors are present in most tissues in men and women, including the brain. The number and sensitivity of the androgen receptors in reproductive and non-reproductive tissues, however, vary based on sex, genetics, and other factors.6

Testosterone Production
Testosterone (T) is produced from cholesterol. Cholesterol might have a bad reputation, but it is the precursor for T, progesterone, cortisol, and all of the steroid hormones that support healthy energy levels, fertility, hair growth, bone health, optimal libido, balanced mood, well-being, and more.
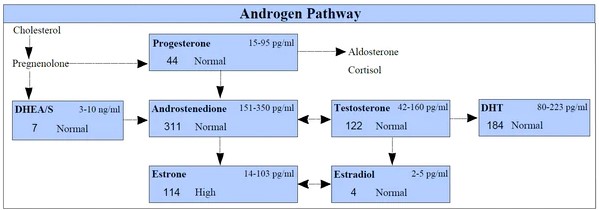
To initiate the process of T production, cholesterol is shuttled into mitochondria and converted into the hormone pregnenolone. Enzymes then convert pregnenolone to either progesterone or DHEA, which are further transformed into androstenedione and androstenediol, the direct precursors of testosterone. Once T is produced, it becomes a precursor for the production of estrogens and the more potent androgen hormone known as dihydrotestosterone (DHT). Roughly 7% of T in healthy men is converted to DHT, and 0.5% of T is converted to estrogen.7
Here is a picture of the Androgen Pathway that shows the production of testosterone and the conversion of testosterone to DHT and Estradiol:
 Testosterone and Fertility
Testosterone and Fertility
In men, testosterone (T) is primarily produced by the Leydig cells in the testes and annex structures. T stimulates the production and maturation of sperm via the activation of the Sertoli cells in the testes.8,9 T is also responsible for the development of male secondary sex characteristics, or the defining characteristics of “maleness,” such as a deep voice.9
In women, T is produced by the ovaries, and T receptors are present in all components of the ovarian follicle, including the granulosa, oocyte, and theca cells.10 The hypothalamus in the brain regulates T production in each ovary by secreting gonadotropin-releasing hormone (GnRH) to stimulate the anterior pituitary to secrete luteinizing hormone (LH).11
The LH then stimulates the theca cells in the ovaries to convert cholesterol into androstenedione and T. The androstenedione and T can be released into circulation or converted to estrogens in the granulosa cells of the ovaries.11
Since T is the precursor for estradiol, T production in the ovary is essential for healthy menstrual cycles and fertility in women. The physiological role of T in women also extends to direct impacts on follicular development. In most women, one egg is released from the dominant follicle during each menstrual cycle. The one follicle most responsive to the pituitary hormone Follicle-Stimulating Hormone (FSH) is the dominant follicle that continues on the path to ovulation. The single, dominant follicle is selected from approximately 5–10 small antral follicles that are recruited during the early follicular phase of the menstrual cycle.10
The other, non-dominant antral follicles are unable to progress and must undergo a phenomenon known as follicular atresia – a type of apoptosis or cell death. According to research, T contributes to follicular atresia, a normal part of healthy follicle maturation.10
The ability of T to modulate atresia in antral follicles has often been considered a pathological, unhealthy effect, particularly in conditions that cause women to have high testosterone levels, such as Polycystic Ovary Syndrome (PCOS). In PCOS, abnormal development of both pre-antral and antral follicles and high T levels are common. But, normal testosterone levels are important for ideal ovarian function, optimal fertility, and healthy follicle development, including follicular atresia.10,12,13

Testosterone and Bone Health
According to research, both increased risk of bone fracture and decreased bone mineral density are associated with age-related testosterone (T) deficiency. The precise mechanisms by which T affects bone density are somewhat unclear, but we know T plays a fundamental role in bone growth and maintenance for both men and women.14
Maintaining bone health while aging, osteoporosis, and osteopenia are significant public health concerns. More women will experience a bone fracture each year than the combined number of women who will experience a stroke, heart attack, or breast cancer.15
Men also experience osteoporotic fractures since osteoporosis is a common condition that afflicts both sexes. The lifetime risk of bone fracture in individuals over 50 years of age is 50% for women and 20% for men. Despite the higher prevalence of osteoporotic fractures in women, osteoporotic fractures in men are more severe and more likely to be associated with disability and death.16
The major factor that contributes to the development of osteoporosis in women is menopause, which is associated with low estrogen levels. In men, age-related testosterone deficiency is the most significant factor that leads to bone loss.15,16
T influences bone health directly by binding to T receptors in bone tissue and indirectly via its conversion to estrogen.16 Research shows T directly stimulates the proliferation of pre-osteoblasts and the differentiation of osteoblasts. Osteoblasts are the specialized bone cells that produce the bone matrix proteins and participate in bone mineralization to strengthen bones.16
Osteoclasts are another type of specialized bone cell. Instead of building bone, the osteoclasts break down bone, which is a process known as “bone resorption.” Studies show T reduces the proliferation of osteoclasts to reduce excessive bone resorption.16
T also affects bone strength indirectly by supporting muscle development. T drives growth and development in both sexes, particularly the accrual, maintenance, and regulation of body protein, including muscle mass. Muscle development is a complex process that is dependent on an adequate supply of dietary energy and protein; and requires many other hormones, such as insulin, growth hormones, and estrogens.9
Bones strengthen based on the amount of force, load, or weight placed on them.17 This is one reason muscle-strengthening and weight-bearing activities are often prescribed to patients who need to improve their bone mineral density.18 Stronger and larger muscles apply more force to the bone, leading to the development of denser and healthier bones.17 T is a crucial regulator of bone mass and overall bone health in men and women.19
 Testosterone and Metabolism
Testosterone and Metabolism
Testosterone plays a key role in carbohydrate, fat, and protein metabolism and significantly influences muscle mass, body fat composition, and systemic energy metabolism.9,20 In men, a LOW T level is associated with obesity, metabolic syndrome, abnormal cholesterol levels, and insulin resistance.9
In women, a HIGH T level is associated with abnormal cholesterol levels, obesity, and insulin resistance.7,21 T also has differing effects on the cardiovascular system in men and women.
 Testosterone and Cardiovascular Health
Testosterone and Cardiovascular Health
In men, a low testosterone (T) level increases the risk of developing and the severity of cardiovascular disease (CVD), including coronary artery disease (CAD) and congestive heart failure (CHF). Low T levels in men are also associated with developing several chronic medical conditions that can increase the risk of developing CVD, including diabetes, hypertension, abnormal cholesterol levels, and renal failure.22
Testosterone replacement therapy in men improves symptoms of CAD; increases exercise capacity in patients with CHF; and decreases blood sugar levels, HbA1c, and insulin resistance in men with diabetes and prediabetes.22
In women, elevated T levels are associated with a potentially increased risk of developing CVD, though the association between an abnormal T level and CVD has not been explored as thoroughly in women. According to several studies, women with higher T levels have higher blood pressure levels. High blood pressure is a significant risk factor for cardiovascular disease.7
 Testosterone and Libido
Testosterone and Libido
Testosterone (T) supports the behavioral changes and the development of the brain structure and function required for reproduction. T activates romantic relationships through complex mechanisms in which cortisol, endorphins, and oxytocin also play important roles. Optimal T production is required for mating and sexual relationships.9
The activation and maintenance of libido are largely controlled by T in men and women. Libido levels in women correlate well with their T levels.9 And clinical studies that assess the effects of T replacement on libido confirm men and women experience a significant improvement when T levels increase.14,23
 Testosterone and Mood
Testosterone and Mood
As a neurosteroid, testosterone (T) does influence mood. According to research, optimal T levels support a good mood and an enjoyable quality of life (QoL).14
QoL is a set of psychological variables, including cognitive and emotional factors, that contribute to an individual’s perception of social, physical, and mental well-being. T plays an important role in the maintenance of QoL. The rates of depression, poor sleep quality, lack of assertiveness, irritability, and dysphoria are higher in men with low T levels.14
Men with low T levels also exhibit a higher rate of fear and anxiety disorders. One study compared free T levels to symptoms of anxiety in over 3400 men. The results of the analysis confirm an inverse association; therefore, the lower the free T level, the more significant the anxiety symptoms.14
In women, the administration of one dose of T significantly reduces anxiety, according to clinical studies.14 Optimal testosterone levels have the potential to improve mood and mental health in both women and men since clinical evidence suggests T has anxiolytic and antidepressant benefits.5
While many think higher T levels increase aggressiveness and anger, research suggests the opposite could be true. Administering reasonable doses of T to men with low T tends to cause a reduction in anger and negative mood.14
But, high doses of anabolic-androgenic steroids, which are structurally similar to T, are known to increase irritability and aggressivity. Thus, the link between T and aggression, violence, and even antisocial behavior, is complex.14
Since both high and low T levels are associated with unpleasant mental health symptoms, it is critically important to monitor the salivary (free) T level in your patients to ensure it is optimal.
 Testosterone and the Immune System
Testosterone and the Immune System
As mentioned above, both a lack and excess of free testosterone (T) may cause adverse effects in many systems, and this includes the immune system. It is well-known that men and women tend to have slightly different immune activity, which appears to be influenced by differences in sex hormone levels. The scientific consensus is that women have more active and robust immune systems compared to men. Therefore, women are better equipped to clear infections but more susceptible to autoimmune diseases.24
T receptors are expressed on many immune cells, including neutrophils, macrophages, and T-cells.25,26 Studies that assessed T levels in men who developed COVID-19 show an association between low T levels and increased symptom severity.27
But, many case studies suggest otherwise healthy men and women who use anabolic-androgenic steroids are at increased risk of developing severe and deadly infections.24 Furthermore, studies that looked at the clinical course of COVID-19 in women with PCOS and high T levels discovered they were more susceptible to the SARS-CoV-2 virus and had more severe symptoms than women with normal T levels.28
The evidence so far suggests that the role of testosterone in Covid‐19 and other infections is a “double‐edged sword” since both high and low T levels appear to contribute to worse outcomes. While the effects of T and anabolic-androgenic steroids on the immune response require more study, the data available to date confirm it is likely best for men and women to maintain optimal free T levels.24
 Testosterone and the Brain
Testosterone and the Brain
Neurons in the brain are affected by testosterone (T) and T metabolites. T increases neuronal survival, stimulates neuronal plasticity and differentiation, and promotes synaptic density and connectivity. T receptors are present on neurons in both the peripheral nervous system and the central nervous system (PNS and CNS).29
In the CNS, T receptors are most concentrated in the hypothalamus. Activation of the T receptors increases the release of brain-derived neurotrophic factor (BDNF), insulin-like growth factor 1 (IGF-1), and vascular endothelial growth factor (VEGF), which support cognitive function, neurogenesis in the brain, and neuroprotective pathways.29
In the PNS, T receptors are present in the neurons in the spinal cord and brainstem. T receptor activation in the PNS is associated with enhanced recovery from damage, extended life span, and enlargement of motor neuron cell bodies. The inhibition or blocking of T receptors leads to neuron degeneration.29
Systematic reviews that assess the effects of androgen deprivation therapy, which is prescribed as a treatment for prostate cancer, have reported an increased risk of dementia, cognitive impairment, and Alzheimer’s disease (AD) in these patients with low T levels. Research shows that those with AD and low T levels have higher plasma β-Amyloid (Aβ) levels. In animal studies, T administration decreases amyloid precursor protein (APP) mRNA and reduces Aβ formation and deposition.29
Researchers suspect T is produced locally in the brain after brain damage and neurodegenerative conditions develop to play neuroprotective and repair roles that regulate the survival and regeneration of brain cells.29
 Both high and low testosterone levels can cause significant health concerns, so consider assessing the salivary (free) testosterone levels in all of your patients. Assessing the bioactive, free hormone level is one advantage of saliva hormone testing; read about additional benefits of testing in our recent article – The Benefits of Saliva Hormone Testing.
Both high and low testosterone levels can cause significant health concerns, so consider assessing the salivary (free) testosterone levels in all of your patients. Assessing the bioactive, free hormone level is one advantage of saliva hormone testing; read about additional benefits of testing in our recent article – The Benefits of Saliva Hormone Testing.
Salivary (free) testosterone can be ordered as part of a:
- Bone Health Panel
- Customized Flexi-Matrix panel
- Male Hormone Panel and Expanded Male Hormone Panel
- Cycling Female Hormone Panel and Expanded Cycling Female Hormone Panel
- Post Menopause Hormone Panel and Expanded Post Menopause Hormone Panel
- Peri Menopause Hormone Panel and Expanded Peri Menopause Hormone Panel
Salivary (free) testosterone can also be ordered as a single test.
To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients. You may select this option at the top of the order form.
Please visit our Provider Tools page for more information about choosing the right test and supporting the androgen pathway.
YOU MAY ALSO ENJOY
April is Stress Awareness Month, so let’s learn more about the stress hormone known as cortisol! While cortisol is known as the stress hormone, it is crucial for the optimal function of your body every day. In healthy individuals, cortisol levels naturally shift throughout the day in a pattern known as a diurnal rhythm.
THE BENEFITS OF SALIVA HORMONE TESTING
If you could choose, would you rather spit into a tube or have a needle jabbed into your arm to measure your hormone levels? We suspect you would rather not get stuck with a needle, and you do have a choice! Saliva hormone testing offers many benefits, including painless collection in the comfort of your home at any time. Saliva hormone tests can help determine the underlying cause(s) of PMS, insomnia, anxiety, fatigue, infertility, migraines, weight gain, hot flashes, hair loss, and many other health concerns.
SYNERGISTIC NUTRIENTS FOR ADRENAL SUPPORT
We often think of supplements as vitamins and minerals that need to be taken only as needed for potential nutrient deficiencies or inadequacies. However, nutritional supplements offer much more and can manifest powerful synergistic benefits that go far beyond simply replacing the vitamins and minerals missing from your diet.
HIDDEN HORMONES IN PERSONAL CARE PRODUCTS
Have you noticed salivary hormone levels trending higher lately? We have certainly noticed this alarming trend in our lab! And we want to let you know we believe it is due to the presence of hidden hormones in personal care products (PCPs). Yes, bioidentical hormones are added to products without being listed as an ingredient. Manufacturers and raw material suppliers are not supposed to add ingredients to products without disclosing them, but; it does occur and seems to be occurring more frequently in recent months, according to our internal data and trends.
References:
- Matfin G. The rejuvenation of testosterone: philosopher’s stone or Brown-Séquard Elixir?. Ther Adv Endocrinol Metab. 2010;1(4):151-154. doi:10.1177/2042018810385052
- Gagliano-Jucá T, Alvarez M, Basaria S. The medicalization of testosterone: reinventing the elixir of life. Rev Endocr Metab Disord. 2022;23(6):1275-1284. doi:10.1007/s11154-022-09751-8
- Pompili A, Iorio C, Gasbarri A. Effects of sex steroid hormones on memory. Acta Neurobiol Exp (Wars). 2020;80(2):117-128.
- Giagulli VA, Lisco G, Mariano F, et al. Is Testosterone the “Fountain of Youth” for Aging Men?. Endocr Metab Immune Disord Drug Targets. 2023;23(2):169-178. doi:10.2174/1871530322666220516160435
- McHenry J, Carrier N, Hull E, Kabbaj M. Sex differences in anxiety and depression: role of testosterone. Front Neuroendocrinol. 2014;35(1):42-57. doi:10.1016/j.yfrne.2013.09.001
- Handelsman DJ. Androgen Physiology, Pharmacology, Use and Misuse. [Updated 2020 Oct 5]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279000/
- Lucas-Herald AK, Touyz RM. Androgens and Androgen Receptors as Determinants of Vascular Sex Differences Across the Lifespan. Can J Cardiol. 2022;38(12):1854-1864. doi:10.1016/j.cjca.2022.09.018
- Witherspoon L, Flannigan R. It puts the T’s in fertility: testosterone and spermatogenesis. Int J Impot Res. 2022;34(7):669-672. doi:10.1038/s41443-022-00531-1
- Alemany M. The Roles of Androgens in Humans: Biology, Metabolic Regulation and Health. Int J Mol Sci. 2022;23(19):11952. doi:10.3390/ijms231911952
- Franks S, Hardy K. Androgen Action in the Ovary. Front Endocrinol (Lausanne). 2018;9:452. doi:10.3389/fendo.2018.00452
- Bienenfeld A, Azarchi S, Lo Sicco K, et al. Androgens in women: Androgen-mediated skin disease and patient evaluation. J Am Acad Dermatol. 2019;80(6):1497-1506. doi:10.1016/j.jaad.2018.08.062
- Neves AR, Montoya-Botero P, Polyzos NP. The Role of Androgen Supplementation in Women With Diminished Ovarian Reserve: Time to Randomize, Not Meta-Analyze. Front Endocrinol (Lausanne). 2021;12:653857. doi:10.3389/fendo.2021.653857
- Walters KA, Handelsman DJ. Role of androgens in the ovary. Mol Cell Endocrinol. 2018;465:36-47. doi:10.1016/j.mce.2017.06.026
- Barone B, Napolitano L, Abate M, et al. The Role of Testosterone in the Elderly: What Do We Know?. Int J Mol Sci. 2022;23(7):3535. doi:10.3390/ijms23073535
- Khosla S, Monroe DG. Regulation of Bone Metabolism by Sex Steroids. Cold Spring Harb Perspect Med. 2018;8(1):a031211. doi:10.1101/cshperspect.a031211
- Mohamad NV, Soelaiman IN, Chin KY. A concise review of testosterone and bone health. Clin Interv Aging. 2016;11:1317-1324. doi:10.2147/CIA.S115472
- Russo V, Chen R, Armamento-Villareal R. Hypogonadism, Type-2 Diabetes Mellitus, and Bone Health: A Narrative Review. Front Endocrinol (Lausanne). 2021;11:607240. doi:10.3389/fendo.2020.607240
- LeBoff MS, Greenspan SL, Insogna KL, et al. The clinician’s guide to prevention and treatment of osteoporosis [published correction appears in Osteoporos Int. 2022 Jul 28;:]. Osteoporos Int. 2022;33(10):2049-2102. doi:10.1007/s00198-021-05900-y
- Corona G, Vena W, Pizzocaro A, et al. Testosterone supplementation and bone parameters: a systematic review and meta-analysis study. J Endocrinol Invest. 2022;45(5):911-926. doi:10.1007/s40618-021-01702-5
- Kelly DM, Jones TH. Testosterone: a metabolic hormone in health and disease. J Endocrinol. 2013;217(3):R25-R45. doi:10.1530/JOE-12-0455
- Yoldemir T. Postmenopausal hyperandrogenism. Climacteric. 2022;25(2):109-117. doi:10.1080/13697137.2021.1915273
- Goodale T, Sadhu A, Petak S, Robbins R. Testosterone and the Heart. Methodist Debakey Cardiovasc J. 2017;13(2):68-72. doi:10.14797/mdcj-13-2-68
- Davis SR, Moreau M, Kroll R, et al. Testosterone for low libido in postmenopausal women not taking estrogen. N Engl J Med. 2008;359(19):2005-2017. doi:10.1056/NEJMoa0707302
- Siserman CV, Jeican II, Gheban D, et al. Fatal Form of COVID-19 in a Young Male Bodybuilder Anabolic Steroid Using: The First Autopsied Case. Medicina (Kaunas). 2022;58(10):1373. doi:10.3390/medicina58101373
- Borkar NA, Combs CK, Sathish V. Sex Steroids Effects on Asthma: A Network Perspective of Immune and Airway Cells. Cells. 2022;11(14):2238. doi:10.3390/cells11142238
- Vancolen S, Sébire G, Robaire B. Influence of androgens on the innate immune system [published online ahead of print, 2023 Feb 25]. Andrology. 2023;10.1111/andr.13416. doi:10.1111/andr.13416
- Yassin A, Sabsigh R, Al-Zoubi RM, et al. Testosterone and Covid-19: An update. Rev Med Virol. 2023;33(1):e2395. doi:10.1002/rmv.2395
- de Medeiros SF, Yamamoto MMW, de Medeiros MAS, et al. Polycystic ovary syndrome and risks for COVID-19 infection: A comprehensive review : PCOS and COVID-19 relationship. Rev Endocr Metab Disord. 2022;23(2):251-264. doi:10.1007/s11154-022-09715-y
- Bianchi VE, Bresciani E, Meanti R, et al. The role of androgens in women’s health and wellbeing. Pharmacol Res. 2021;171:105758. doi:10.1016/j.phrs.2021.105758