 Tapeworm Infection – Neurocysticercosis (NCC) Symptoms
Tapeworm Infection – Neurocysticercosis (NCC) Symptoms
Neurocysticercosis (NCC), characterized by the presence of cysticerci in the nervous system, is the deadliest form of a Taenia solium infection. Research suggests that up to 56% of all epilepsy cases in developing countries are caused by NCC, and it is frequently fatal due to surgical complications.1
According to Gonzales et al., based on imaging studies, the vast majority of individuals with NCC do not develop noticeable symptoms; however, the presence of pericystic inflammation is typically associated with symptoms.2,3
NCC is considered a great mimicker of many other diseases.4 The most common signs and symptoms of NCC include seizures, focal impairments, and headaches; however, the size, location, and number of larvae present in the nervous system can cause significant variations in the clinical presentation of patients with NCC.1
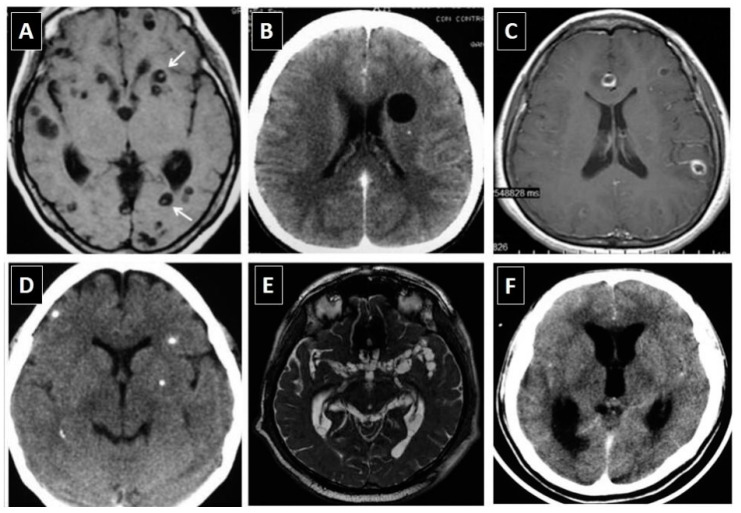 Image Source: Neuroimaging characteristics of neurocysticercosis
Image Source: Neuroimaging characteristics of neurocysticercosis
Additional signs and symptoms of NCC may include, but are not limited to:
- Acute Psychosis
- Agitation
- Mutism
- Disorganized behavior
- Persecutory delusions5
- Anxiety5,6
- Depression5,7
- Depression is present in 36 to 85% of NCC cases and the most commonly described psychiatric manifestation.
- Proinflammatory cytokines, such as IFN-g, IFN-a, IL-1b, and TNF-a, have been implicated in the pathogenesis of depression.
- A decrease in hippocampal volume is a well-documented finding in depression and calcified NCC has been associated with hippocampal atrophy.
- Stimulation of the hypothalamic-hypophysis-adrenal (HPA) axis by altering negative feedback mechanisms could play a role.
- The prevalence of depression in patients with epilepsy and calcified NCC is higher than that found in patients with epilepsy due to other causes.
- Research suggests that depression does not seem to be directly related to infection burden or disease stage.3
- Personality disorders7
- Dementia can occur in up to 12% of patients with NCC.3,7
- Inflammation could play a role in the development of Taenia-associated dementia because cognitive decline is more significant in patients with active NCC compared to those with only calcified lesions.
- Experimental models suggest that NCC might compromise short-term memory by altering hippocampal physiology via inflammatory cytokines, such as TNF-a and IFN-g.
- Cognitive impairment is present in up to 87.5% of patients with NCC.3
- Lymphocytosis
- Hallucinations
- Paranoia5
- Stuttering (dysphemia)4
- Akathisia, restlessness4,5
- Space occupying lesion (SOL), leading to mass effects
- Papilledema
- Convulsions2
- Optic neuropathy with blurring of vision and other symptoms2,8
- Hemiparesis
- Cranial nerve deficits9
- Vomiting10
- Mechanical obstruction of cerebrospinal fluid (CSF) outflow, leading to hydrocephalus8,11
- Intracranial hypertension
- Meningitis11
- Suprapubic pain with urinary retention
- Bilateral cortical blindness, loss of vision
- Fatigue
- Fever
- Encephalitis
- Slurred speech
- Confusion
- Hemiplegia with loss of sensation (sensory deficits)
- Extraparenchymal NCC vasculitis
- Inflammatory occlusion of the arteries at the brainstem due to arachnoiditis
- Arterial compression, leading to a stroke (infarction)
- Extrapyramidal symptoms
- Hemiballismus
- Dorsal midbrain syndrome
- Aphasia
- Pleocytosis with eosinophilia and a high protein level in the CSF12
- Monoparesis
- Weakness and spasticity in extremities
- Tremor
- Paresthesia
- Hyperreflexia
- Brainstem compression
- Bruns syndrome5
- Parkinsonism
- Ataxia
- Chorea
- Dystonia
- Myokymia
- Myoclonus
- Ballism
- Tics
- Dyskinesia
- Paraparesis
- Quadriparesis
- Neck pain
- Limb pain
- Back pain
- Cauda-equina syndrome13
- Schizoaffective symptoms14
- Dysarthria
- Panic attacks
- Suicidal ideation
- Sudden behavioral changes15
After diagnosis and treatment, periodic MRI assessments should be repeated every six months until the resolution of the cystic lesions.8
More information is available at these links:
- Diagnose Taeniasis (Tapeworm Infection) – Stool Test for Intestinal Parasites – DiagnosTechs, Inc.
- Symptoms of Taeniasis (Taenia solium Infection) – DiagnosTechs, Inc.
- Best Stool Test for Intestinal Parasites – DiagnosTechs, Inc.
- Is It A Worm? Is It A Parasite? TEST – Don’t Guess! – DiagnosTechs, Inc.
- Taenia solium (Tapeworm) Treatment Protocols
- Complete GI Parasite List
- Resources on Diagnosis of Parasitic Diseases
- Tapeworm (Taenia solium) Treatment – Taeniasis, Cysticercosis, and Neurocysticercosis (NCC) – DiagnosTechs, Inc.
- Tapeworm (Taenia solium) Infection Prevention – DiagnosTechs, Inc.
- How Common Are Tapeworms (Taenia solium) in the US? – DiagnosTechs, Inc.
- Saliva Screening Test for Taeniasis, Cysticercosis, and Neurocysticercosis (NCC) – DiagnosTechs, Inc.
- Tapeworm (Taenia solium) Infection – Cysticercosis Symptoms – DiagnosTechs, Inc.
To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients.
 References:
References:
- Kusnoto K, Khairullah AR, Sunarso A, et al. The hidden threat of cysticercosis: A neglected public health problem. Open Vet J. 2025;15(3):1101-1115. doi:10.5455/OVJ.2025.v15.i3.4
- Bandyopadhyay D, Sen S. Disseminated cysticercosis with huge muscle hypertrophy. Indian J Dermatol. 2009;54(1):49-51. doi:10.4103/0019-5154.48987
- Gonzales I, Rivera JT, Garcia HH; Cysticercosis Working Group in Peru. Pathogenesis of Taenia solium taeniasis and cysticercosis. Parasite Immunol. 2016;38(3):136-146. doi:10.1111/pim.12307
- Rissardo JP, Caprara ALF, Durante Í. Neurocysticercosis and movement disorders: A literature review. Brain Circ. 2020;6(4):225-241. doi:10.4103/bc.bc_48_20
- Alfahal MS, Jalkhi T. Calcified frontal neurocysticercosis presenting with acute psychosis in a non-endemic context: a case report. Front Psychiatry. 2026;17:1771798. doi:10.3389/fpsyt.2026.1771798
- Govindani NP Sr, Gaikwad HM. Frontal Lobe Neurocysticercosis Presenting With Seizures and Anxiety: A Case Report Highlighting Radiological-Psychological Dimensions. Cureus. 2025;17(11):e97015. doi:10.7759/cureus.97015
- El-Kady AM, Allemailem KS, Almatroudi A, et al. Psychiatric Disorders of Neurocysticercosis: Narrative Review. Neuropsychiatr Dis Treat. 2021;17:1599-1610. doi:10.2147/NDT.S306585
- Vaibhav, Sharma R, Aggarwal HK, et al. Neurocysticercosis-Induced Monoparesis: A Case Report of a Rare Neurological Manifestation. Cureus. 2024;16(6):e62587. doi:10.7759/cureus.62587
- Stelzle D, Makasi CE, Schmidt V, et al. Evaluation of a point-of-care test for the diagnosis of Taenia solium neurocysticercosis in rural southern Tanzania: a diagnostic accuracy study. Lancet Infect Dis. 2024;24(1):98-106. doi:10.1016/S1473-3099(23)00378-X
- López-Hernández A, Garaizar C. Childhood cerebral cysticercosis: clinical features and computed tomographic findings in 89 Mexican children. Can J Neurol Sci. 1982;9(4):401-407. doi:10.1017/s0317167100044309
- García-Martínez CE, Scatularo CE, Farina JM, et al. Cysticercosis & Heart: A Systematic Review. Curr Probl Cardiol. 2023;48(8):101195. doi:10.1016/j.cpcardiol.2022.101195
- Opara NU. Cortical Blindness Due to Neurocysticercosis in an Adolescent Patient. Trop Med Infect Dis. 2022;7(6):96. doi:10.3390/tropicalmed7060096
- Garg RK, Rizvi I, Nigam H, et al. Treatment outcome in patients with spinal neurocysticercosis: a systematic review of published cases and case series. Future Microbiol. 2025;20(1):45-56. doi:10.1080/17460913.2024.2428526
- Annor E, Lee G, Kelly S, et al. Frontal Lobe Neurocysticercosis Presenting With Schizoaffective Symptoms in an Adolescent Immigrant. Cureus. 2025;17(9):e92071. doi:10.7759/cureus.92071
- Azevedo S, Pereira S, Vilar da Mota R, et al. The Pathological Fear of COVID-19 and Neuroparasitosis: A Case Report of Neurocysticercosis. Cureus. 2025;17(1):e77655. doi:10.7759/cureus.77655