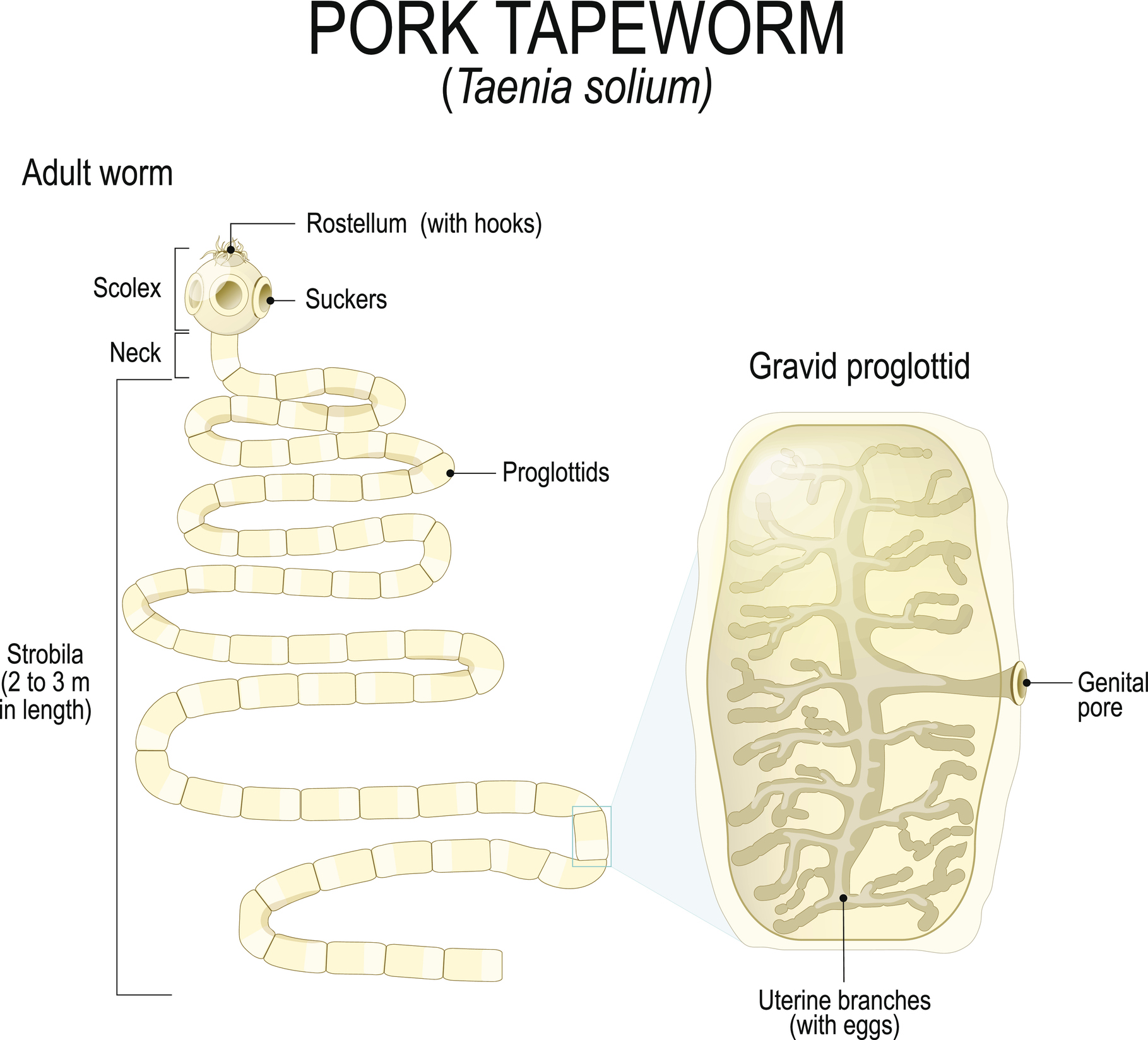
 How Common Are Tapeworms (Taenia solium) in the US?
How Common Are Tapeworms (Taenia solium) in the US?
According to research, parasitic infections could be more common in some areas of the United States than healthcare providers acknowledge. According to the results of a population-based study published in 2008, the overall prevalence of taeniasis in Texas along the border with Mexico was 3%. Taeniasis was diagnosed based on the presence of Taenia spp. in a stool sample during the study.1
A more recent study published in 2010 reported that an active Taenia spp. infection was present in a total of 3.3% of study participants near the US-Mexico border. Alarmingly, an infection with Taenia spp. was more common on the U.S. side of the border. A surprising 9.7% – nearly 10% – of participants in El Paso, TX tested positive for active taeniasis compared with only 1.1% of participants in Ciudad Juarez, Mexico. Overall, individuals living in El Paso, TX were approximately 8.6 times more likely to test positive for taeniasis than those living in Mexico.2
 Diagnostic Testing for a Tapeworm Infection in the Intestinal Tract (Taeniasis)
Diagnostic Testing for a Tapeworm Infection in the Intestinal Tract (Taeniasis)
Testing is indicated for all patients in the US and other countries who present with signs or symptoms that could be caused by an infection with Taenia solium. The gold standard test for the diagnosis of most intestinal parasites is the Ova & Parasites times three or “O & P x 3” test.3
DiagnosTechs offers microscopic and macroscopic testing for the diagnosis of taeniasis. The O & P x 3 test can be ordered as a standalone GP2B – Ova and parasites, three samples test or as part of the GP9S – Comprehensive Ova and Parasites Panel™ and the GP10S – Extended Comprehensive Ova and Parasites Panel™.
The DiagnosTechs GP1G – GI parasite, gross exam test can also be ordered for the gross macroscopic examination of a worm or worm segment (proglottid) collected from a stool sample when a patient reports seeing them. Ensure that precautions are always taken when handling a stool sample to prevent the contamination of surfaces and infection.
While stool microscopy and macroscopic examination are the optimal tests to diagnose taeniasis, false negatives are possible since eggs, proglottids, and adult parasites are not excreted with every bowel movement. Furthermore, eggs and proglottids are not released into the feces until approximately 2 to 3 months after the adult tapeworm is established in the upper jejunum. Therefore, repeated examination and the stool microscopy concentration techniques used by DiagnosTechs laboratory will increase the likelihood of detecting new or light infections.3
 Saliva Screening Test for Tapeworm – Taeniasis, Cysticercosis, and Neurocysticercosis (NCC)
Saliva Screening Test for Tapeworm – Taeniasis, Cysticercosis, and Neurocysticercosis (NCC)
Taenia solium is present in developed and developing countries throughout the world, including the United States, and anyone can be affected. A 20-month-old child from Minnesota, who had no history of international travel or pork consumption, was diagnosed with neurocysticercosis (NCC), according to a case report published in 2005. The authors suggest that NCC must be considered and ruled out in any child with nonfebrile seizures in the US because exposure to international travelers has become so common.4
Moreover, NCC is the most common cause of adult-acquired epilepsy worldwide.5 The incidence of NCC ranges from approximately 1.5 to 5.8 cases per 100,000 individuals in the US. The highest prevalence is observed among Hispanic immigrants, and individuals who have either immigrated from or traveled to endemic areas. Cities with large immigrant populations, such as Los Angeles, Houston, and New York City, report a significantly higher number of NCC cases.6
Depression, anxiety, or other symptoms associated with neurocysticercosis suggest the need for a Taenia solium screening test, at the very least. The unique and non-invasive DiagnosTechs T-SOL Taenia solium (tapeworm) antibody, sIgA saliva test screens for a mucosal immune response to Taenia solium.
The larvae penetrate the walls of the GI tract to cause cysticercosis and neurocysticercosis, which could elicit a clinically detectable immune response in serum, saliva, and CSF.7-10
Secretory IgA (sIgA) Antibody Screening Test Result Interpretation
Additional assessment to diagnose a current infection with Taenia solium is required when the saliva antibody test is positive since it is not a diagnostic test. Moreover, antibody detection does not indicate active cysticercosis or taeniasis is present since antibody production can result from exposure alone in the absence of an acute infection. Furthermore, the lifespan of Taenia-specific antibodies varies and depends on the immune history of the host and the burden or severity of infection. Therefore, antibodies can remain elevated long after successful treatment, leading to a false positive test result.11
A false negative test result is possible during acute taeniasis due to the limited contact between the intestinal tapeworm and the mucosal tissue, potentially leading to a muted inflammatory response.11
Further testing is required if the T-SOL saliva antibody test is negative but symptoms are consistent with a diagnosis of taeniasis, cysticercosis, or neurocysticercosis.
Further assessment could include the DiagnosTechs GP2B stool microscopy test, imaging, biopsy, serum antibody testing, endoscopy, electromyography, and other tests as indicated based on the clinical presentation of the patient and latest diagnostic guidelines.12,13
More information is available at these links:
- Diagnose Taeniasis (Tapeworm Infection) – Stool Test for Intestinal Parasites – DiagnosTechs, Inc.
- Symptoms of Taeniasis (Taenia solium Infection) – DiagnosTechs, Inc.
- Best Stool Test for Intestinal Parasites – DiagnosTechs, Inc.
- Is It A Worm? Is It A Parasite? TEST – Don’t Guess! – DiagnosTechs, Inc.
- Taenia solium (Tapeworm) Treatment Protocols
- Complete GI Parasite List
- Resources on Diagnosis of Parasitic Diseases
- Tapeworm (Taenia solium) Treatment – Taeniasis, Cysticercosis, and Neurocysticercosis (NCC) – DiagnosTechs, Inc.
- Tapeworm (Taenia solium) Infection Prevention – DiagnosTechs, Inc.
- Saliva Screening Test for Taeniasis, Cysticercosis, and Neurocysticercosis (NCC) – DiagnosTechs, Inc.
- Tapeworm (Taenia solium) Infection – Cysticercosis Symptoms – DiagnosTechs, Inc.
- Tapeworm Infection – Neurocysticercosis (NCC) Symptoms – DiagnosTechs, Inc.
To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients.
 References:
References:
- Barton Behravesh C, Mayberry LF, Bristol JR, et al. Population-based survey of taeniasis along the United States-Mexico border. Ann Trop Med Parasitol. 2008;102(4):325-333. doi:10.1179/136485908X300788
- Cardenas VM, Mena KD, Ortiz M, et al. Hyperendemic pylori and tapeworm infections in a U.S.-Mexico border population. Public Health Rep. 2010;125(3):441-447. doi:10.1177/003335491012500313
- CDC – DPDx – Taeniasis. Centers for Disease Control and Prevention. June 7, 2024. Accessed April 28, 2026. https://www.cdc.gov/dpdx/taeniasis/index.html.
- Mody R, Nield LS, Stauffer W, Kamat D. Seizures in a 20-month-old native of Minnesota: a case of neurocysticercosis. Pediatr Emerg Care. 2005;21(12):860-862. doi:10.1097/01.pec.0000190232.20233.45
- Opara NU. Cortical Blindness Due to Neurocysticercosis in an Adolescent Patient. Trop Med Infect Dis. 2022;7(6):96. doi:10.3390/tropicalmed7060096
- Osorio Borjas M, Hernandez RJ, Lopez-Lacayo A, et al. Echoes of Dormancy: Anomic Aphasia Unveils Neurocysticercosis Reactivation in a Patient on Semaglutide. NeuroSci. 2025;6(2):40. doi:10.3390/neurosci6020040
- Flisser A, Plancarte A, Correa D, et al. New approaches in the diagnosis of Taenia solium cysticercosis and taeniasis. Ann Parasitol Hum Comp. 1990;65 Suppl 1:95-98. doi:10.1051/parasite/1990651095
- Saha R, Roy P, Das S, et al. Anti-cysticercus antibody detection in saliva as a potential diagnostic tool for neurocysticercosis. Ann Indian Acad Neurol. 2016;19(3):414-416. doi:10.4103/0972-2327.179972
- Feldman M, Plancarte A, Sandoval M, et al. Comparison of two assays (EIA and EITB) and two samples (saliva and serum) for the diagnosis of neurocysticercosis. Trans R Soc Trop Med Hyg. 1990;84(4):559-562. doi:10.1016/0035-9203(90)90040-l
- Acosta E. Antibodies to the metacestode of Taenia solium in the saliva from patients with neurocysticercosis. J Clin Lab Anal. 1990;4(2):90-94. doi:10.1002/jcla.1860040204
- Lesh EJ, Brady MF. Tapeworm. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537154/
- Bandyopadhyay D, Sen S. Disseminated cysticercosis with huge muscle hypertrophy. Indian J Dermatol. 2009;54(1):49-51. doi:10.4103/0019-5154.48987
- El-Kady AM, Allemailem KS, Almatroudi A, et al. Psychiatric Disorders of Neurocysticercosis: Narrative Review. Neuropsychiatr Dis Treat. 2021;17:1599-1610. doi:10.2147/NDT.S306585