 Tapeworm (Taenia solium) Infection – Symptoms, Diagnosis & Treatment
Tapeworm (Taenia solium) Infection – Symptoms, Diagnosis & Treatment
A tapeworm infection can cause symptoms from head to toe, including neuropsychiatric symptoms, such as anxiety, depression, paranoia, behavioral changes, and psychosis. The symptoms associated with a tapeworm infection can vary significantly and depend on the type of infection and the location(s) of the tapeworms in the body.
There are two types of Taenia solium (tapeworm) infections that can develop based on the route of transmission. If the eggs from an adult worm, which are expelled in human and animal feces, are ingested, cysticerci develop in tissues and cause cysticercosis. If cysticerci develop in the central nervous system (CNS), the condition is called neurocysticercosis.1
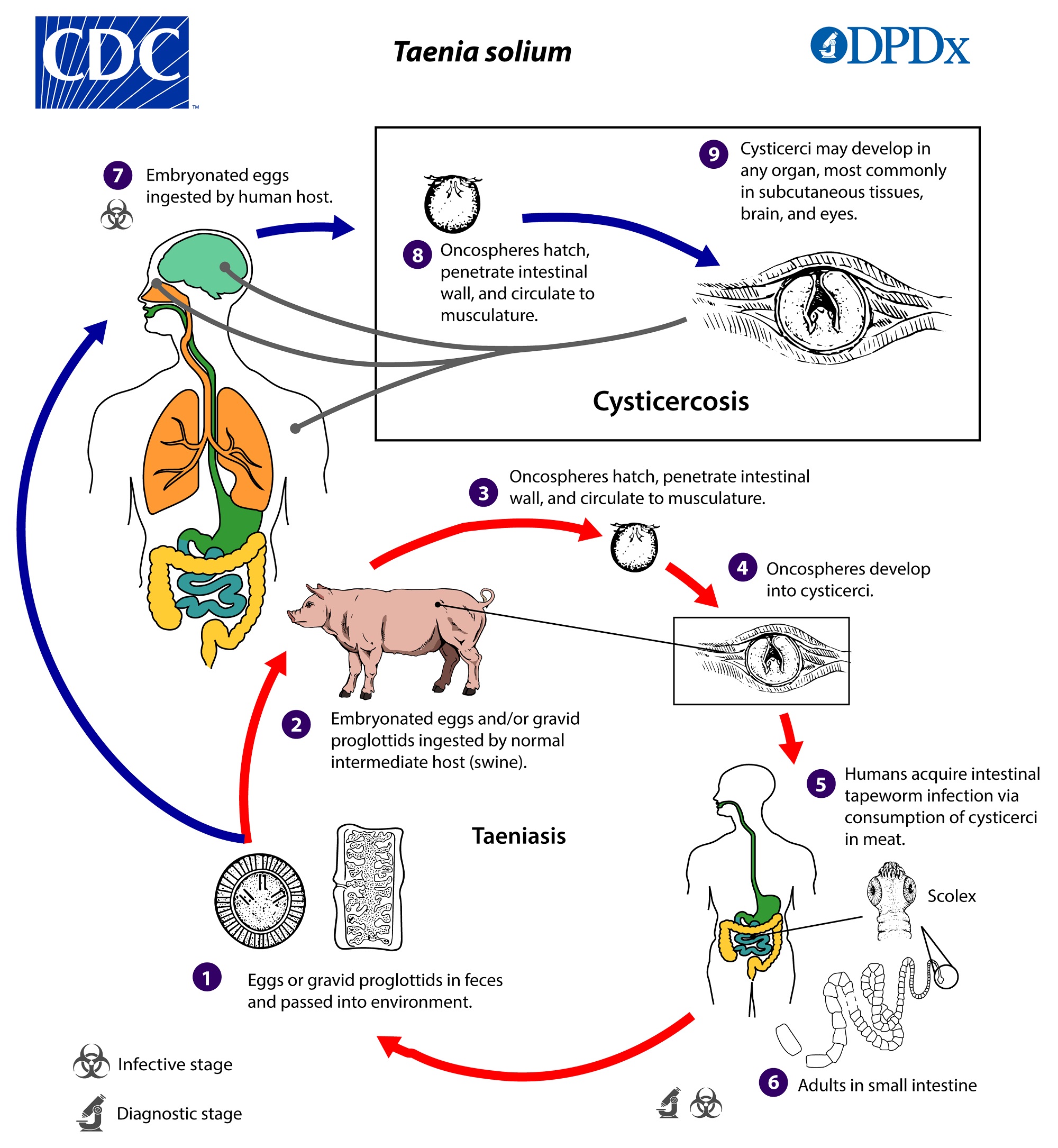
Image Source: CDC – DPDx – Cysticercosis
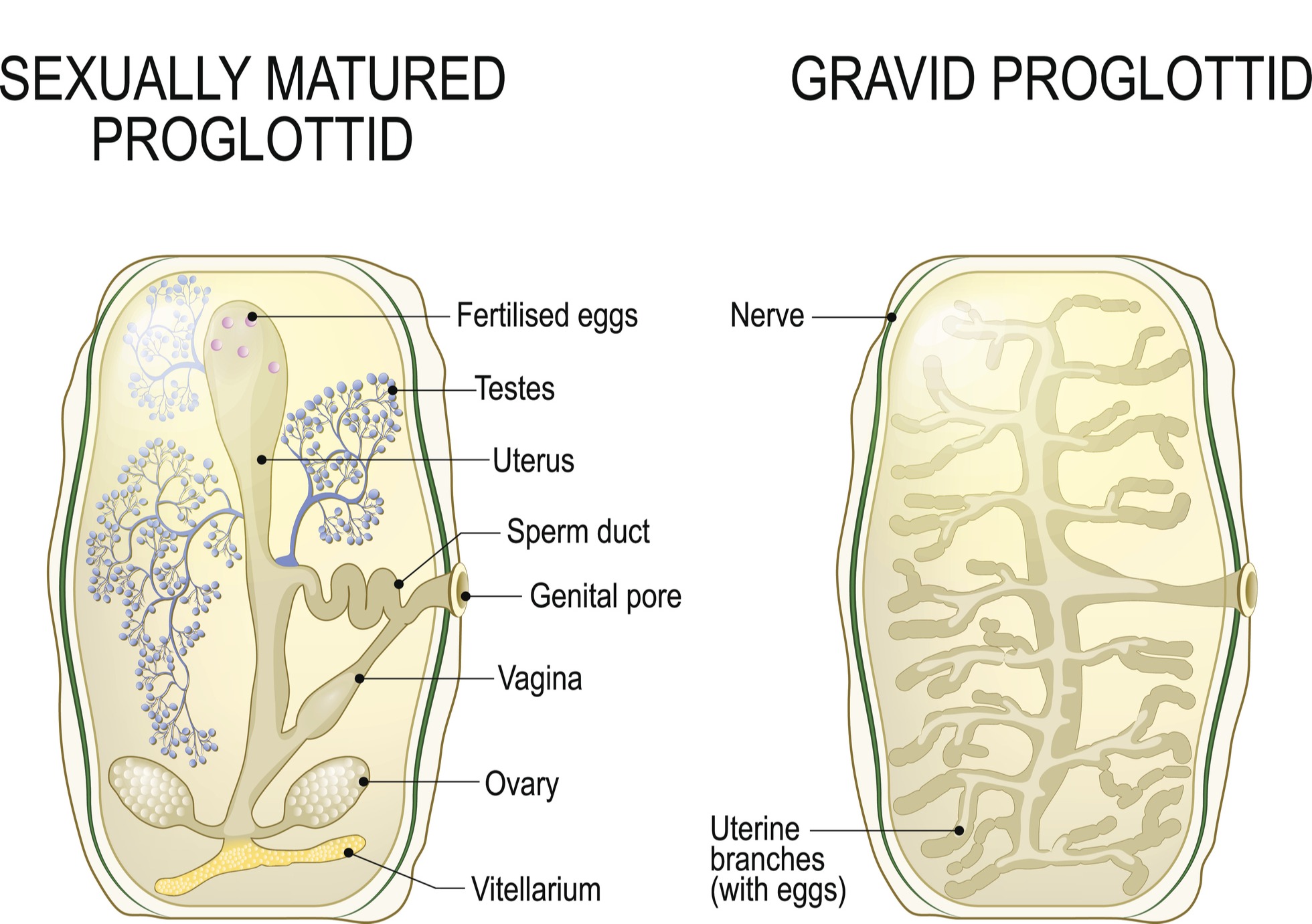
An adult tapeworm can be seen without a microscope and grow to a length of 2 – 7 meters. One mature, adult tapeworm can release hundreds of proglottids (worm segments), each of which contains roughly 50,000 eggs, and is also visible without a microscope.2
A tapeworm can live in the host for up to 25 years while releasing gravid proglottids with infectious eggs. Research suggests that autoinfection and person-to-person spread occur more often than previously suspected, and millions are infected globally.1,2 Taeniasis in humans causes cysticercosis and neurocysticercosis via fecal-oral transmission secondary to autoinfection, environmental contamination, and person-to-person contact.
DiagnosTechs offers a test to quickly and definitively diagnose taeniasis, as well as a unique and non-invasive saliva antibody test to screen for exposure and an immune response to Taenia solium.
 Tapeworm Infection – Taeniasis Symptoms
Tapeworm Infection – Taeniasis Symptoms
Taeniasis, an infection of the gastrointestinal tract that occurs after consuming raw or undercooked pork with viable tapeworm cysts, can be asymptomatic or cause mild symptoms, such as anal pruritus due to the passage of the proglottids and abdominal discomfort. In general, children tend to be more symptomatic than adults.1
 Other symptoms of taeniasis may include:
Other symptoms of taeniasis may include:
- Nausea
- Changes in appetite (both increased and decreased appetite have been reported)
- Weakness
- Weight loss
- Headache
- Constipation
- Dizziness
- Diarrhea
- Eosinophilia1
- Colicky abdominal pain
- Malnutrition3
Rare complications of taeniasis may also occur, including intestinal, biliary, or pancreatic obstruction, which can cause severe symptoms and require surgical intervention.1,4
Gravid proglottids in the stool are visible to the naked eye; therefore, many patients first become aware of a tapeworm infection after noticing the sesame seed or rice-like proglottids after a bowel movement.1 The proglottids in the stool can be motile, though it is typically the proglottids of the beef tapeworm, Taenia saginata, that are motile, rather than Taenia solium, the pork tapeworm.3,5 Rarely, patients may also regurgitate or aspirate a proglottid, leading to other symptoms.1
The minimal symptoms observed in most patients could be due to the limited contact between the intestinal tapeworm and the mucosal tissue, resulting in a muted inflammatory response.1 Despite minimal symptoms, it is imperative to diagnose and treat taeniasis as quickly as possible because taeniasis can cause cysticercosis and neurocysticercosis. Therefore, identifying and treating cases of taeniasis expediently may prevent life-threatening cases of neurocysticercosis and cysticercosis in the household and community.6
 Tapeworm Infection – Cysticercosis Symptoms
Tapeworm Infection – Cysticercosis Symptoms
Cysticercosis is caused by ingesting the eggs of Taenia solium, the pork tapeworm. After the consumption of eggs or a gravid proglottid, the eggs hatch into larvae, which are distributed systemically via the blood after penetrating the walls of the GI tract.7 The larvae can lodge in various tissues, including the skin, skeletal muscles, eyes, spleen, pancreas, and heart, to cause cysticercosis. Cysticercosis severity can range from asymptomatic to life-threatening.7,8
Signs and symptoms of cysticercosis depend on the location of the larvae and may include:
- Soft lumps beneath the skin2
- Pseudohypertrophy of muscles7,8
- Cardiovascular signs and symptoms:
- Chest pain
- Palpitations
- Arrhythmias
- Cardiac conduction disturbances
- Pericardial effusion
- Heart failure
- Syncope
- Shortness of breath
- Cardiac valve dysfunction9
- Myocarditis10
- Arterial hypertension10,11
- Ocular cysticercosis signs and symptoms:
- Subconjunctival cysts
- Subretinal cysts
- Papilledema
- Atypical optic neuritis
- Lid nodules
- Intraretinal cysts12
- Proptosis with restricted ocular movements9,12
- Vision changes9
- Loss of vision
- Periorbital redness and swelling13
- Deviations in gaze14
When the cysticerci affect the muscles, the clinical presentation can be of the myalgic type, nodular type or the uncommon pseudohypertrophic type. A rare condition known as ‘disseminated muscular cysticercosis syndrome’ is characterized by muscular pseudohypertrophy, palpable subcutaneous nodules, and seizures with abnormal mentation. The muscles affected by pseudohypertrophy are generally nontender.7
While the most common clinical presentations involve the nervous and musculoskeletal systems, up to 25% of cases of cysticercosis cases can involve the cardiovascular system. Cardiac cysticercosis is often asymptomatic; however, it can present with severe symptoms, including sustained ventricular tachycardia. Fortunately, timely and appropriate anthelmintic treatment combined with corticosteroids can be curative, even in cases of cardiac cysticercosis.9
Cysticercosis is associated with early mortality, morbidity, and disability. Roughly 20 million individuals suffer from T. solium cysticercosis globally, leading to approximately 50,000 deaths each year. And, as more people migrate from regions where T. solium is endemic, the prevalence of cysticercosis continues to increase in developed nations.2 Morbidity is most commonly caused by the involvement of the eyes or CNS.7 Neurocysticercosis in the CNS is the deadliest form of tapeworm infection, and discussed in more detail below.2
 Tapeworm Infection – Neurocysticercosis (NCC) Symptoms
Tapeworm Infection – Neurocysticercosis (NCC) Symptoms
Neurocysticercosis (NCC), characterized by the presence of cysticerci in the nervous system, is the deadliest form of a Taenia solium infection. Research suggests that up to 56% of all epilepsy cases in developing countries are caused by NCC, and it is frequently fatal due to surgical complications.2
According to Gonzales et al., based on imaging studies, the vast majority of individuals with NCC do not develop noticeable symptoms; however, the presence of pericystic inflammation is typically associated with symptoms.7,14
NCC is considered a great mimicker of many other diseases.15 The most common signs and symptoms of NCC include seizures, focal impairments, and headaches; however, the size, location, and number of larvae present in the nervous system can cause significant variations in the clinical presentation of patients with NCC.2
Additional signs and symptoms of NCC may include, but are not limited to:
- Space occupying lesion (SOL), leading to mass effects
- Papilledema
- Convulsions7
- Optic neuropathy with blurring of vision and other symptoms7,12
- Hemiparesis
- Cranial nerve deficits16
- Dementia can occur in up to 12% of patients with NCC.
- Inflammation could play a role in the development of Taenia-associated dementia because cognitive decline is more significant in patients with active NCC compared with those with only calcified lesions.
- Experimental models suggest that NCC might compromise short-term memory by altering hippocampal physiology via inflammatory cytokines, such as TNF-a and IFN-g.
- Cognitive impairment does not seem to be associated with the numbers or locations of NCC lesions.
- Cognitive impairment is present in up to 87.5% of patients with NCC.14
- Vomiting11
- Mechanical obstruction of cerebrospinal fluid (CSF) outflow, leading to hydrocephalus 9,12
- Intracranial hypertension9
- Meningitis9
- Suprapubic pain with urinary retention
- Bilateral cortical blindness, loss of vision
- Fatigue
- Fever
- Encephalitis
- Slurred speech
- Confusion
- Hemiplegia with loss of sensation (sensory deficits)
- Extraparenchymal NCC vasculitis
- Inflammatory occlusion of the arteries at the brainstem due to arachnoiditis
- Arterial compression, leading to a stroke (infarction)
- Extrapyramidal symptoms
- Hemiballismus
- Dorsal midbrain syndrome
- Aphasia
- Pleocytosis with eosinophilia and high protein level in the CSF17
- Monoparesis
- Weakness and spasticity in extremities
- Tremor
- Paresthesia
- Hyperreflexia
- Brainstem compression
- Bruns syndrome12
- Parkinsonism
- Ataxia
- Chorea
- Dystonia
- Myokymia
- Myoclonus
- Ballism
- Tics
- Dyskinesia
- Stuttering (dysphemia)15
- Akathisia, restlessness15,18
- Lymphocytosis
- Hallucinations
- Paranoia
- Acute Psychosis
- Agitation
- Mutism
- Disorganized behavior
- Persecutory delusions18
- Anxiety18,19
- Depression18,20
- Depression is present in 36 to 85% of NCC cases and the most commonly described psychiatric manifestation.
- Proinflammatory cytokines, such as IFN-g, IFN-a, IL-1b, and TNF-a, have been implicated in the pathogenesis of depression.
- A decrease in hippocampal volume is a well-documented finding in depression and calcified NCC has been associated with hippocampal atrophy.
- Stimulation of the hypothalamic-hypophysis-adrenal (HPA) axis by altering negative feedback mechanisms could play a role.
- The prevalence of depression in patients with epilepsy and calcified NCC is higher than that found in patients with epilepsy due to other causes.
- Research suggests that depression does not seem to be directly related to infection burden or disease stage.14
- Personality disorders
- Dementia20
- Paraparesis
- Quadriparesis
- Neck pain
- Limb pain
- Back pain
- Cauda-equina syndrome21
- Schizoaffective symptoms22
- Dysarthria
- Panic attacks
- Suicidal ideation
- Sudden behavioral changes23
After diagnosis and treatment, periodic MRI assessments should be repeated every six months until the resolution of the cystic lesions.12
 Stool Microscopy Test for Taeniasis (Tapeworm Infection) Diagnosis
Stool Microscopy Test for Taeniasis (Tapeworm Infection) Diagnosis
While many healthcare providers believe that parasitic infections are exceptionally rare in the United States, some research suggests otherwise. According to a population-based study published in 2008, the overall prevalence of taeniasis, diagnosed based on the presence of Taenia spp. in stool samples, in Texas along the border with Mexico was 3%.24
A more recent study published in 2010 reported that an active Taenia spp. infection was present in a total of 3.3% of study participants near the US-Mexico border. Alarmingly, an infection with Taenia spp. was more common on the U.S. side of the border. A surprising 9.7% – yes, nearly 10% – of participants in El Paso, TX tested positive for active taeniasis compared with only 1.1% of participants in Ciudad Juarez, Mexico.25
 Testing is indicated for all patients in the US and other countries who present with signs or symptoms that could be caused by an infection with Taenia solium. The gold standard test for the diagnosis of most intestinal parasites is the Ova & Parasites times three or “O & P x 3” test.26
Testing is indicated for all patients in the US and other countries who present with signs or symptoms that could be caused by an infection with Taenia solium. The gold standard test for the diagnosis of most intestinal parasites is the Ova & Parasites times three or “O & P x 3” test.26
The O & P x 3 test can be ordered from DiagnosTechs Laboratory as a standalone GP2B – Ova and parasites, three samples test or as part of the GP9S – Comprehensive Ova and Parasites Panel™ and the GP10S – Extended Comprehensive Ova and Parasites Panel™. DiagnosTechs offers both microscopic and macroscopic testing for the diagnosis of taeniasis.
The DiagnosTechs GP1G – GI parasite, gross exam test can be ordered for the gross macroscopic examination of a worm or worm segment (proglottid) collected from a stool sample when a patient reports seeing them. Ensure that precautions are always taken when handling a stool sample to prevent the contamination of surfaces and infection.
While stool microscopy and macroscopic examination are the optimal tests to diagnose taeniasis, false negatives are possible since eggs, proglottids, and adult parasites are not excreted with every bowel movement. Furthermore, eggs and proglottids are not released into the feces until approximately 2 to 3 months after the adult tapeworm is established in the upper jejunum. Therefore, repeated examination and the stool microscopy concentration techniques used by DiagnosTechs laboratory will increase the likelihood of detecting new or light infections.26
 Saliva Screening Test for Taeniasis, Cysticercosis, and Neurocysticercosis (NCC)
Saliva Screening Test for Taeniasis, Cysticercosis, and Neurocysticercosis (NCC)
Taenia solium is present in developed and developing countries throughout the world, including the United States, and anyone can be affected. A 20-month-old child from Minnesota, who had no history of international travel or pork consumption, was diagnosed with neurocysticercosis, according to a case report published in 2005. The authors suggest that neurocysticercosis must be considered and ruled out in any child with nonfebrile seizures in the US because exposure to international travelers is increasingly common.27
Moreover, NCC is the most common cause of adult-acquired epilepsy worldwide.17 The incidence of NCC ranges from approximately 1.5 to 5.8 cases per 100,000 individuals in the US. The highest prevalence is observed among Hispanic immigrants, and individuals who have either immigrated from or traveled to endemic areas. Cities with large immigrant populations, such as Los Angeles, Houston, and New York City, report a significantly higher number of NCC cases.28
The presence of depression, anxiety, or other symptoms associated with neurocysticercosis suggest that a Taenia solium screening test could be ordered. The unique and non-invasive DiagnosTechs T-SOL Taenia solium (tapeworm) antibody, sIgA saliva test screens for a mucosal immune response to Taenia solium. The larvae penetrate the walls of the GI tract and enter the systemic circulation to cause cysticercosis and neurocysticercosis, which can elicit a clinically detectable immune response in serum, saliva, and CSF.29-32
Please note that a false negative test result is also possible during acute taeniasis due to the limited contact between the intestinal tapeworm and the mucosal tissue, potentially leading to a muted inflammatory response.1 Further testing is required if the T-SOL saliva antibody test is negative but the patient’s symptoms are consistent with a diagnosis of taeniasis, cysticercosis, or neurocysticercosis.
Additional assessment to diagnose a current infection with Taenia solium is also indicated when the saliva antibody test is positive since the saliva antibody test is not a diagnostic test. Moreover, antibody detection does not confirm that active cysticercosis or taeniasis is present since antibody production can result from exposure alone in the absence of an acute infection. Furthermore, the lifespan of Taenia-specific antibodies varies and depends on the immune history of the host and the burden or severity of infection. Therefore, antibodies can remain elevated after successful treatment.1
Further assessment could include the DiagnosTechs GP2B stool microscopy test, imaging, biopsy, serum antibody testing, endoscopy, electromyography, and other tests as indicated based on the clinical presentation of the patient and diagnostic guidelines.7,20
 Prevention of Tapeworm (Taenia solium) Infection
Prevention of Tapeworm (Taenia solium) Infection
Although Taenia solium has a global distribution, the highest prevalence is found in areas with poor access to adequate clean water and sanitation. Prevalence can also be high in populations that ingest raw or undercooked meat. At this time, prevalence is highest in Africa, Asia, Latin America, Eastern Europe, China, Pakistan, and India. Due to diagnostic limitations in certain areas, the true prevalence could be higher than current estimates.1
Infections can be prevented with strategies that target all potential hosts. Humans are both definitive and intermediate hosts for Taenia solium, while pigs serve as intermediate hosts. Therefore, all pigs that have a tapeworm infection were infected by a human with taeniasis. Humans with taeniasis can cause cysticercosis in pigs, themselves, and other humans.2,5
 To prevent Taenia solium infections, consider implementing these strategies:
To prevent Taenia solium infections, consider implementing these strategies:
- Test everyone with signs or symptoms of taeniasis.
- Treat and confirm eradication in all patients who test positive for a tapeworm infection.
- Wash your hands thoroughly with hot, soapy water after using the restroom and before and after handling food.
- Wash all raw fruits and vegetables thoroughly.
- Properly cook foods, especially pork and vegetables.9
- Ground pork must be cooked to an internal temperature of 160 °F (71 ºC), according to Michigan State University.
- Pork roasts, pork chops, pork ribs, and other cuts must be cooked to an internal temperature of at least 150 ºF (65 ºC).1
- Neither pickling nor salt-curing pork ensures infection prevention.1
- Use an accurate meat thermometer to test for doneness in the middle of the thickest part, ensuring safety.33
- Freezing pork at a temperature of 23 ºF (-5 ºC) for at least 4 days kills cysticerci.34
- Separate raw meat, poultry, seafood, and eggs from other foods and each other.
- Designate a cutting board for fresh produce and a separate one for raw meat, poultry, and seafood. Never use the same cutting board for all foods.
- Never place cooked food on a plate or in an area that previously held raw food, including meat, poultry, seafood, eggs, or raw vegetables.
- Once a marinade or sauce has touched raw meat, bring it to a boil before consuming.
- Store meat properly.
- Refrigerate or freeze it as soon as possible.
- Keep it cold at 40 °F or below when stored in a refrigerator.
- Keep the meat hot at 135 °F or above until serving.
- Never let raw meat sit at room temperature for more than two hours.
- Never defrost meat at room temperature. Instead, thaw meat in the refrigerator, submerged in cold water, or in the microwave, and then cook immediately after thawing.33
- Ensure that preventive measures, including inspection, vaccination, and treatment, are complete and up-to-date on pig farms.35,36
 Cysticercosis, Neurocysticercosis (NCC), and Taeniasis Disease Treatment
Cysticercosis, Neurocysticercosis (NCC), and Taeniasis Disease Treatment
In general, if a lesion could be present in the nervous system or eyes, ocular cysticercosis, intraventricular NCC, massive/encephalitic NCC, and lesions in the brainstem and other high-risk areas must be ruled out before pharmacotherapy is initiated. Precautions must always be taken before and during the treatment of NCC to prevent adverse events, especially in patients with intracranial hypertension secondary to NCC.6
The diagnosis of NCC can be challenging, even with imaging. The differential for multiple ring-enhancing lesions of the brain is broad and includes bacterial abscess, tuberculosis, syphilis, toxoplasmosis, echinococcosis, multiple sclerosis (MS), coccidioidomycosis, cryptococcosis, aspergillosis, neoplastic metastasis, CNS lymphoma, and sarcoidosis.1
Please note that there is never an urgent need for pharmacotherapy for patients with NCC. Moreover, the NCC treatment plan must always be individualized after the number and locations of lesions are determined. Ideally, patients with NCC will be managed by an experienced and multidisciplinary team of qualified healthcare professionals, including specialists in infectious disease, neuroradiology, neurology, pediatrics, and neurosurgery.6
Symptoms, including seizures and headaches, should be managed until it is safe to consider surgery and or antiparasitic medications. Treatment of NCC with antiparasitic medications must always be performed under medical supervision for at least one week. The medications must also be administered with concomitant steroid therapy to prevent adverse events and preceded by appropriate symptomatic treatment.6
Once NCC is ruled out or managed appropriately concomitantly, treatment for taeniasis or cysticercosis can be prescribed. Pharmaceutical treatment options are noted in the document Taenia solium (Tapeworm) Treatment Protocols, which is posted on the Provider Tools page in the Provider Portal.
One animal study suggests that progesterone could be protective and open the door for the treatment of gastrointestinal helminth infections via the immunoendocrinological network.37,38 Ensure that saliva (free) steroid hormone levels, including progesterone, are optimal.
 The most important goal when treating taeniasis is the prevention of NCC and cysticercosis. Therefore, eradication must be confirmed with extensive follow-up testing after treatment. According to the guidelines recommended by the international and interdisciplinary expert group known as COHEMI, microscopic and macroscopic examination of stool samples repeated on three different days at one and three months after treatment should be ordered. If a test result is positive, the treatment protocol and additional follow-up testing must be repeated until all follow-up testing is negative.6
The most important goal when treating taeniasis is the prevention of NCC and cysticercosis. Therefore, eradication must be confirmed with extensive follow-up testing after treatment. According to the guidelines recommended by the international and interdisciplinary expert group known as COHEMI, microscopic and macroscopic examination of stool samples repeated on three different days at one and three months after treatment should be ordered. If a test result is positive, the treatment protocol and additional follow-up testing must be repeated until all follow-up testing is negative.6
Testing other household members, discussing and implementing all food safety guidelines, initiating preventive strategies, and ruling out a chronic, ongoing exposure to a source of Taenia solium could also be indicated when the first round of taeniasis treatment fails.
Infection with Taenia solium is a significant danger to human health and livestock production.13 Fortunately, readily available and affordable screening and diagnostic testing from DiagnosTechs can help facilitate the treatment of current infections and the prevention of future infections.
More information is available at these links:
- How Common Are Tapeworms (Taenia solium) in the US? – DiagnosTechs, Inc.
- Best Stool Test for Intestinal Parasites – DiagnosTechs, Inc.
- Is It A Worm? Is It A Parasite? TEST – Don’t Guess! – DiagnosTechs, Inc.
- Taenia solium (Tapeworm) Treatment Protocols
- Complete GI Parasite List
- Resources on Diagnosis of Parasitic Diseases
To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients.
 References:
References:
- Lesh EJ, Brady MF. Tapeworm. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537154/
- Kusnoto K, Khairullah AR, Sunarso A, et al. The hidden threat of cysticercosis: A neglected public health problem. Open Vet J. 2025;15(3):1101-1115. doi:10.5455/OVJ.2025.v15.i3.4
- Kandi V, Moses VK. Taeniasis Presenting as Motile Worms in the Stools: An Emerging but Neglected Parasitic Disease. Cureus. 2022;14(10):e30066. doi:10.7759/cureus.30066
- Yu HJ, Ahn CS, Lim S, et al. Biliary Taeniasis with Cholecystitis: An Unusual Case of Taenia solium Infection with a Literature Review. Am J Trop Med Hyg. 2019;100(1):135-139. doi:10.4269/ajtmh.18-0633
- García HH, Gonzalez AE, Evans CA, Gilman RH; Cysticercosis Working Group in Peru. Taenia solium cysticercosis. Lancet. 2003;362(9383):547-556. doi:10.1016/S0140-6736(03)14117-7
- Zammarchi L, Bonati M, Strohmeyer M, et al. Screening, diagnosis and management of human cysticercosis and Taenia solium taeniasis: technical recommendations by the COHEMI project study group. Trop Med Int Health. 2017;22(7):881-894. doi:10.1111/tmi.12887
- Bandyopadhyay D, Sen S. Disseminated cysticercosis with huge muscle hypertrophy. Indian J Dermatol. 2009;54(1):49-51. doi:10.4103/0019-5154.48987
- Vaidya A, Singhal S, Dhall S, et al. Asymptomatic disseminated cysticercosis. J Clin Diagn Res. 2013;7(8):1761-1763. doi:10.7860/JCDR/2013/5465.3269
- García-Martínez CE, Scatularo CE, Farina JM, et al. Cysticercosis & Heart: A Systematic Review. Curr Probl Cardiol. 2023;48(8):101195. doi:10.1016/j.cpcardiol.2022.101195
- Shogan PJ, Yasmer JF, Monson M. Cardiac cysticercosis. AJR Am J Roentgenol. 2009;192(5):W212-W213. doi:10.2214/AJR.08.2000
- López-Hernández A, Garaizar C. Childhood cerebral cysticercosis: clinical features and computed tomographic findings in 89 Mexican children. Can J Neurol Sci. 1982;9(4):401-407. doi:10.1017/s0317167100044309
- Vaibhav, Sharma R, Aggarwal HK, et al. Neurocysticercosis-Induced Monoparesis: A Case Report of a Rare Neurological Manifestation. Cureus. 2024;16(6):e62587. doi:10.7759/cureus.62587
- Shen ZZ, Luo HQ. Changing Trends in the Cysticercosis-Related Disease Burden from 1990 to 2021 and its Predicted Level in 2022-2050 Years. Acta Parasitol. 2025;70(3):118. doi:10.1007/s11686-025-01058-3
- Gonzales I, Rivera JT, Garcia HH; Cysticercosis Working Group in Peru. Pathogenesis of Taenia solium taeniasis and cysticercosis. Parasite Immunol. 2016;38(3):136-146. doi:10.1111/pim.12307
- Rissardo JP, Caprara ALF, Durante Í. Neurocysticercosis and movement disorders: A literature review. Brain Circ. 2020;6(4):225-241. doi:10.4103/bc.bc_48_20
- Stelzle D, Makasi CE, Schmidt V, et al. Evaluation of a point-of-care test for the diagnosis of Taenia solium neurocysticercosis in rural southern Tanzania: a diagnostic accuracy study. Lancet Infect Dis. 2024;24(1):98-106. doi:10.1016/S1473-3099(23)00378-X
- Opara NU. Cortical Blindness Due to Neurocysticercosis in an Adolescent Patient. Trop Med Infect Dis. 2022;7(6):96. doi:10.3390/tropicalmed7060096
- Alfahal MS, Jalkhi T. Calcified frontal neurocysticercosis presenting with acute psychosis in a non-endemic context: a case report. Front Psychiatry. 2026;17:1771798. doi:10.3389/fpsyt.2026.1771798
- Govindani NP Sr, Gaikwad HM. Frontal Lobe Neurocysticercosis Presenting With Seizures and Anxiety: A Case Report Highlighting Radiological-Psychological Dimensions. Cureus. 2025;17(11):e97015. doi:10.7759/cureus.97015
- El-Kady AM, Allemailem KS, Almatroudi A, et al. Psychiatric Disorders of Neurocysticercosis: Narrative Review. Neuropsychiatr Dis Treat. 2021;17:1599-1610. doi:10.2147/NDT.S306585
- Garg RK, Rizvi I, Nigam H, et al. Treatment outcome in patients with spinal neurocysticercosis: a systematic review of published cases and case series. Future Microbiol. 2025;20(1):45-56. doi:10.1080/17460913.2024.2428526
- Annor E, Lee G, Kelly S, et al. Frontal Lobe Neurocysticercosis Presenting With Schizoaffective Symptoms in an Adolescent Immigrant. Cureus. 2025;17(9):e92071. doi:10.7759/cureus.92071
- Azevedo S, Pereira S, Vilar da Mota R, et al. The Pathological Fear of COVID-19 and Neuroparasitosis: A Case Report of Neurocysticercosis. Cureus. 2025;17(1):e77655. doi:10.7759/cureus.77655
- Barton Behravesh C, Mayberry LF, Bristol JR, et al. Population-based survey of taeniasis along the United States-Mexico border. Ann Trop Med Parasitol. 2008;102(4):325-333. doi:10.1179/136485908X300788
- Cardenas VM, Mena KD, Ortiz M, et al. Hyperendemic pylori and tapeworm infections in a U.S.-Mexico border population. Public Health Rep. 2010;125(3):441-447. doi:10.1177/003335491012500313
- CDC – DPDx – Taeniasis. Centers for Disease Control and Prevention. June 7, 2024. Accessed April 28, 2026. https://www.cdc.gov/dpdx/taeniasis/index.html.
- Mody R, Nield LS, Stauffer W, Kamat D. Seizures in a 20-month-old native of Minnesota: a case of neurocysticercosis. Pediatr Emerg Care. 2005;21(12):860-862. doi:10.1097/01.pec.0000190232.20233.45
- Osorio Borjas M, Hernandez RJ, Lopez-Lacayo A, et al. Echoes of Dormancy: Anomic Aphasia Unveils Neurocysticercosis Reactivation in a Patient on Semaglutide. NeuroSci. 2025;6(2):40. doi:10.3390/neurosci6020040
- Flisser A, Plancarte A, Correa D, et al. New approaches in the diagnosis of Taenia solium cysticercosis and taeniasis. Ann Parasitol Hum Comp. 1990;65 Suppl 1:95-98. doi:10.1051/parasite/1990651095
- Saha R, Roy P, Das S, et al. Anti-cysticercus antibody detection in saliva as a potential diagnostic tool for neurocysticercosis. Ann Indian Acad Neurol. 2016;19(3):414-416. doi:10.4103/0972-2327.179972
- Feldman M, Plancarte A, Sandoval M, et al. Comparison of two assays (EIA and EITB) and two samples (saliva and serum) for the diagnosis of neurocysticercosis. Trans R Soc Trop Med Hyg. 1990;84(4):559-562. doi:10.1016/0035-9203(90)90040-l
- Acosta E. Antibodies to the metacestode of Taenia solium in the saliva from patients with neurocysticercosis. J Clin Lab Anal. 1990;4(2):90-94. doi:10.1002/jcla.1860040204
- Pork Safety. Pork.org. April 10, 2024. Accessed May 6, 2026. https://pork.org/pork-safety/.
- Sotelo J, Rosas N, Palencia G. Freezing of infested pork muscle kills cysticerci. JAMA. 1986;256(7):893-894.
- Promoting prevention and control of Taenia solium infection through animals with the one health approach. World Health Organization. Accessed April 29, 2026. https://www.who.int/activities/promoting-prevention-and-control-of-taenia-solium-infection-through-animals-with-the-one-health-approach.
- Okello AL, Thomas LF. Human taeniasis: current insights into prevention and management strategies in endemic countries. Risk Manag Healthc Policy. 2017;10:107-116. doi:10.2147/RMHP.S116545
- Escobedo G, Camacho-Arroyo I, Nava-Luna P, et al. Progesterone induces mucosal immunity in a rodent model of human taeniosis by Taenia solium. Int J Biol Sci. 2011;7(9):1443-1456. doi:10.7150/ijbs.7.1443
- Terrazas LI, Satoskar AR, Morales-Montor J, Rodriguez-Sosa M. Innate and cellular immunology in parasitic diseases. Int J Biol Sci. 2011;7(9):1216-1219. doi:10.7150/ijbs.7.1216